Journal Volume 1 - January 2006
Article 11
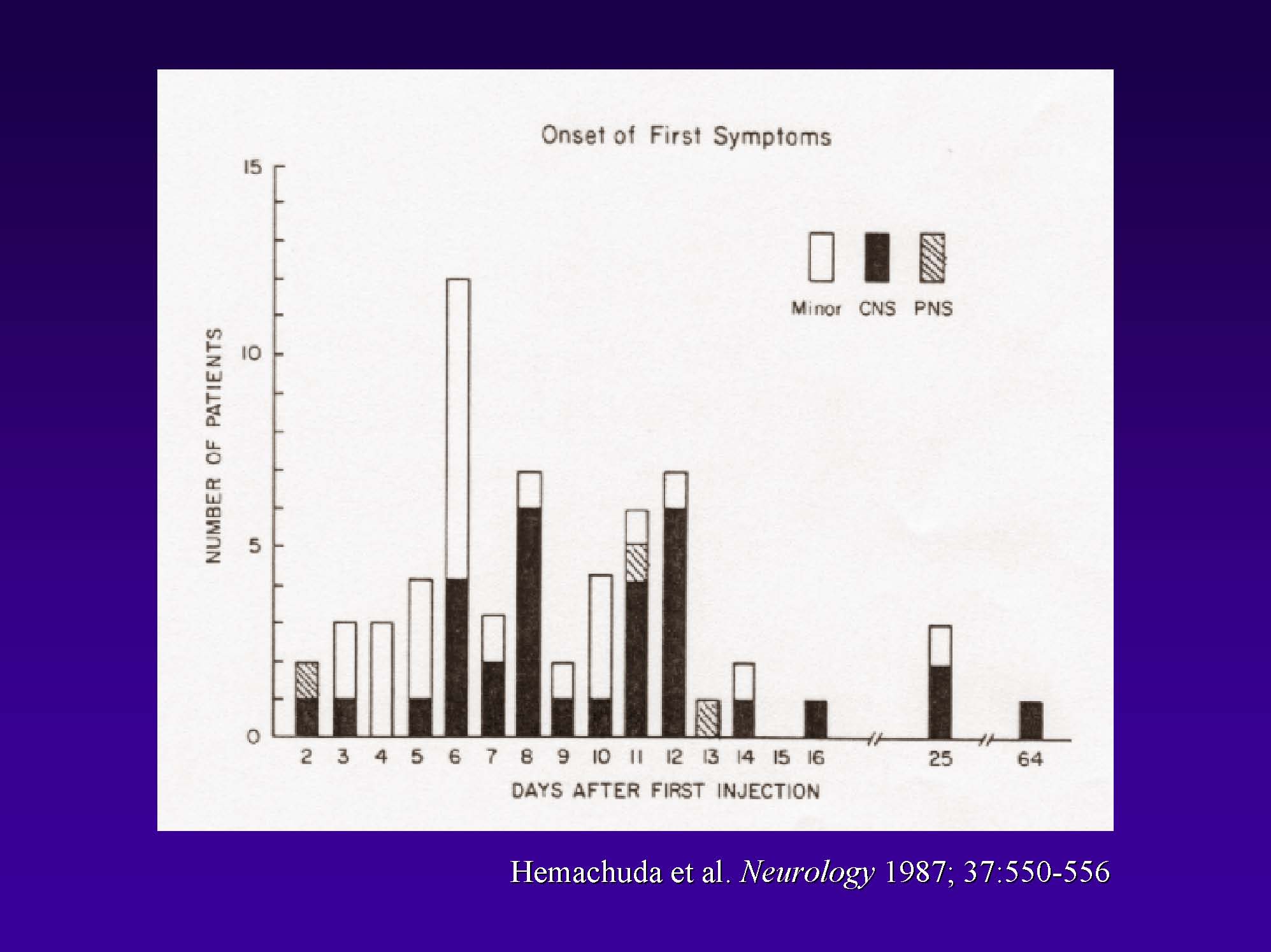
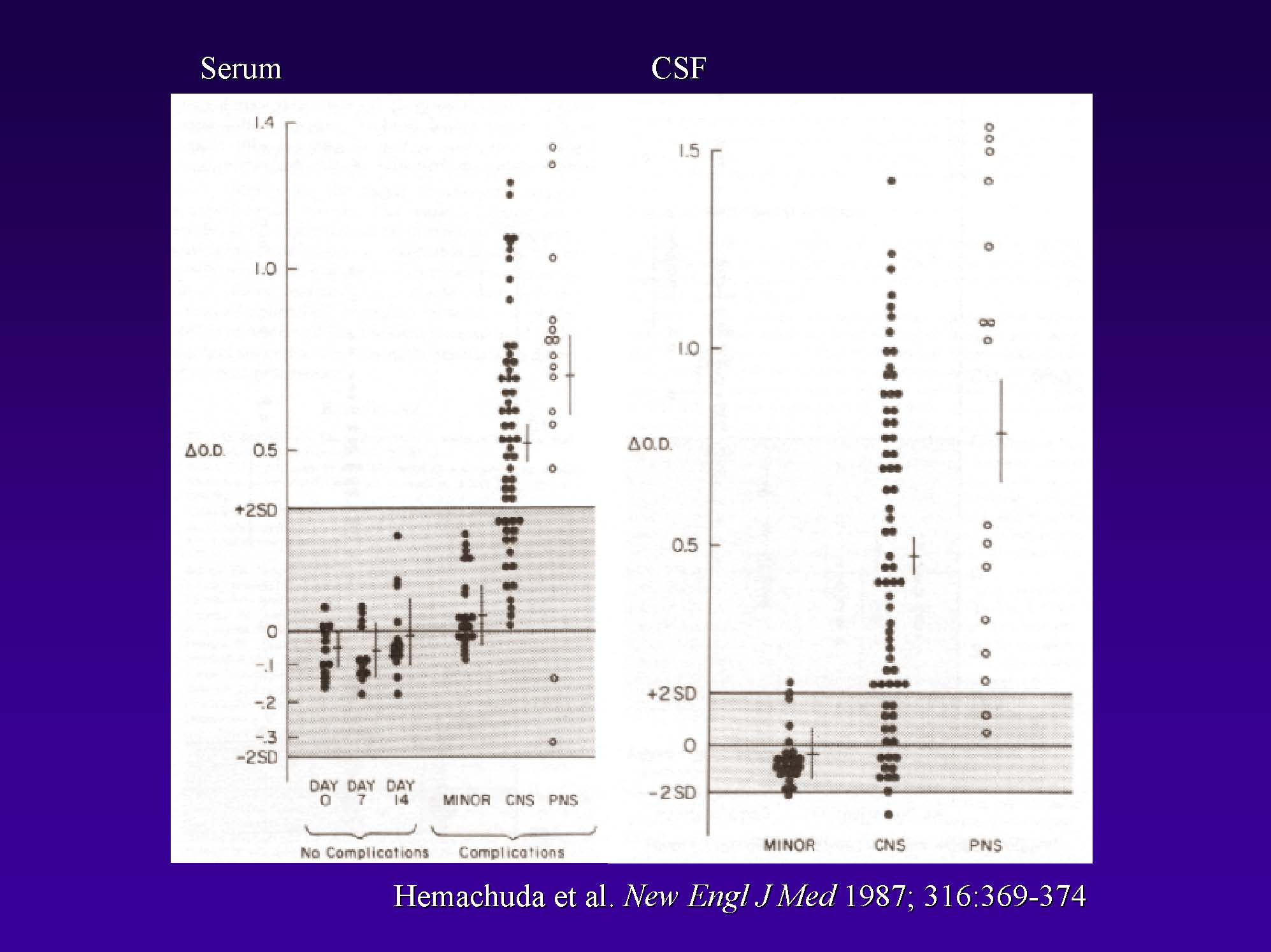
Neuroimmunological Lessons Learned from Acute Disseminated Encephalomyelitis Introduction This paper will review a group of disorders collectively referred to as acute disseminated encephalomyelitis (ADEM). In particular, I will focus on the issue of what might trigger this disease. While there may be some people who are more likely to get these diseases than others (i.e., a genetic susceptibility), the genetics by itself does not tell the whole story. Indeed, there is very likely something that triggers ADEM in susceptible individuals. In particular, there are certain infectious diseases and particular vaccines that have been shown to precipitate inflammatory demyelination in the central nervous system (CNS). I am going to talk about two in some immunological detail. There are many schemes used to categorize inflammatory demyelinating diseases of the CNS (i.e., the brain and spinal cord). Multiple sclerosis (MS) is a longitudinal disease with symptoms that come and go in a relapsing-remitting pattern. ADEM, on the other hand, typically is a monophasic disease; that is, it occurs as a one-time event. Still, ADEM is multifocal in that it typically affects multiple parts of the nervous system when it happens. More site-restricted monofocal disorders such as transverse myelitis (TM) can occur where the immune attack occurs predominately or exclusively in one location of the CNS (in this case, the spinal cord). Thus, there exists a whole spectrum of CNS inflammatory disorders, of which ADEM is only a small part. Keep in mind there also is an animal model of CNS inflammatory demyelination called experimental autoimmune encephalomyelitis (EAE). Many scientists study this disease from an immunological standpoint. We hope these studies will educate us as to what might be happening in human inflammatory demyelinating diseases. ADEM: Clinical Definitions and Features ADEM is characterized by inflammation and demyelination within the CNS. Symptoms are typically quite rapid in onset, with pediatric and adult patients often getting sick over a period of a few days. This results in focal or multifocal neurological dysfunction. Furthermore, many cases of ADEM occur immediately following an infection or on the heels of certain vaccinations. Having said this, it is critically important at this point to make clear that this is not a message that I think vaccines are unsafe. Vaccine science is a very advanced field, and the vaccines used today are extremely safe products. I am not advocating that patients avoid getting vaccinations! Indeed, the vaccine I am going to cite as an example of one trigger for ADEM is not in use any more. This example simply makes some immunological points that I want to bring out, so I will describe it in some detail. Finally, it should be remembered that there are occasional examples of ADEM which are chronic illnesses or that come back with recurrences. This, however, is a small minority of cases. ADEM: Diagnosis So, how do we diagnose this disorder? There is a great need to develop more rigorous and uniform diagnostic criteria for these rare neuroimmunological disorders. ADEM is a perfect example of that need. We currently do not have a single test that identifies this disease. The diagnosis is facilitated by taking a careful patient history with particular attention about what happened in the time immediately preceding the onset of neurological symptoms, particularly with reference to antecedent infections and recent vaccinations or immunizations. The physical and neurological examination demonstrates evidence of involvement in more than one part of the CNS. Beyond this, magnetic resonance imaging (MRI) is an invaluable tool in helping identify patients with ADEM. The lesions of myelin, predominately in the white matter, but also in the gray matter, show up very readily on MRI scans (Figure 1). Even though the lesion pattern can be very different from one patient to another, there are general MRI patterns that help us identify and diagnose this disease. Finally, we commonly analyze the cerebrospinal fluid (CSF) by doing a lumbar puncture to look for evidence of immune overactivity within the CNS; too many white blood cells and/or elevated levels of certain immune proteins in the CSF are important clues. Putting these pieces of information together helps us arrive at a diagnosis. Beyond these tests and procedures, we often rely on the response to therapy as another helpful tool to decide whether the patient really has ADEM or not. Many patients are given corticosteroid treatments intravenously in the acute phase of the illness to try and reduce suspected CNS inflammation and to facilitate recovery. We want to get this inflammation under control as quickly as possible to minimize any collateral damage to nerves and their myelin coverings, and to maximize the chance of clinical recovery. Finally, following patients over time in terms of their clinical and MRI features is very helpful in clarifying the diagnosis over time. The above images are an example of the MRI findings in a patient who developed ADEM following a vaccination. This is actually a patient from Thailand who developed ADEM after receiving the older form of the rabies vaccine (the so-called Semple vaccine). The point here is that the lesions in the white matter show up as white patches on the three MRI scans. This patient also had very prominent involvement in the cervical spinal cord with this high signal intensity. These lesions can develop in multiple parts of the nervous system simultaneously, and the MRI is very useful in identifying the lesions and clarifying the diagnosis. Differentiating ADEM from MS When looking at an MRI scan, it can be very difficult to distinguish a patient with ADEM from someone who has MS. The location and orientation of the multiple lesions can be very similar between the two conditions. One quandary we often face is whether the clinical symptoms we are observing in the patient actually represent the first attack of MS (i.e., symptoms that will turn out to return in a relapsing-remitting pattern), or are a single isolated event that may recover and not come back, as in most cases of ADEM. Differentiating ADEM from multiple sclerosis can be very difficult (Figure 2). ADEM will remain difficult to diagnose and to differentiate from MS based on MRI scans alone. Only through a better understanding of the molecular mechanisms involved in these diseases will we be able to develop tests that will more reliably distinguish these two conditions. For example, I predict that there are subtle differences in the types of proteins that are present in the CSF of patients that will eventually help us to distinguish ADEM from MS. ADEM: Precipitating Events At this point, I now want to focus on the events that we think may precipitate or trigger an ADEM attack. If we can better understand what activates the immune system in ADEM, this may teach us valuable lessons that will carry over into the understanding of other neuroimmunological disorders. As mentioned, the two most common events associated with the onset of ADEM are recent infections and certain recent vaccinations. Be aware, however, that some investigators have reported that ADEM can follow treatment with certain medications, can occur on the heels of trauma, and can develop with absolutely no precipitating cause (idiopathic ADEM). Since we do not have a very good understanding of these triggers, I will not discuss them any more here. Neurologic Complications of the Semple Rabies Vaccine The history of rabies vaccination goes back to the late 1880’s and the time of Louis Pasteur. It was Pasteur who first determined that he could prevent overt rabies in someone who had been bitten by a rabid animal by injecting that patient with brain or spinal cord tissue from an animal known to have had rabies. This was one of the very earliest demonstrations of vaccination. In essence, he was training the immune system of the exposed patient to respond to rabies virus in the vaccine in order to prevent the actual disease to which that person had been exposed. The problem, of course, is that when you inject rabies-infected CNS tissue into a patient, you may actually transmit the disease itself. That was the main drawback of Pasteur’s approach. In 1911, however, David Semple developed the technique of phenol-inactivation of live rabies virus in animal brain tissue. He figured out that you could inject this material into humans and still effectively prevent the development of rabies with little risk of disease transmission. This vaccine was easy and inexpensive to make, and it was readily available for use in the developing world where rabies is common. Beginning in the 1920’s, it became clear that when you injected a tissue homogenate of spinal cord or brain tissue into a human, patients occasionally developed neurological complications from the vaccine. These so-called “neuroparalytic accidents” have since been best studied in the developing world, particularly in Thailand, where rabies is common. The CNS inflammatory disease is referred to as SAE – Semple Vaccine-Induced Autoimmune Encephalomyelitis. From the period of 1961 to 1970, one out of every four hundred patients who received the Semple rabies vaccine developed an inflammatory demyelinating disease soon thereafter (156 cases out of 59,597 vaccines in Bangkok, Thailand). That 1:400 complication rate is absolutely unacceptable by today’s standards as a vaccine. We would not tolerate a flu vaccine or a hepatitis vaccine that caused this degree of disease. That is why this vaccine is no longer used. But this case is very instructive. Investigators were able to identify 61 patients who developed SAE between April 1984 and June 1985. The disease manifested itself in a variety of forms. Of these 61 cases, 36 developed major neurological complications, including encephalitis, myelitis, polyradiculitis, or meningitis. On the other hand, 25 had minor complications, including headache, fever, inflamed injection sites but had normal CSF. Blood samples were taken for immunological studies in comparison to patients who received the vaccine that did not get these complications. They used this comparative approach to try and understand what was being triggered by the vaccine to cause the disease. SAE developed relatively soon after the vaccine was given, and not months later. This is the same as post-infectious encephalomyelitis; it is something that happens as the infection is waning, not something that crops up months or years after an infection. (Figure 3) In terms of the outcome from this disease, SAE usually was a fairly short-lived illness. The duration of the disease in the majority of the patients studied in this paper had lasted a week or two, although a small subset had a more chronic disease and there was one patient who actually had a relapsing-remitting pattern. Like other forms of ADEM, this was a one-time disease that came, produced neurological symptoms, and resolved itself, either partially or completely. Many patients actually made a complete recovery, although some did not. (Figure 4) Now, I am going to discuss the neuroimmunology of these SAE patients. It turns out that when you inject nervous system tissue into a human, you can prime that person’s immune system to respond to myelin proteins that are present in that homogenate. One of the best studied myelin proteins is called myelin basic protein (MBP), a normal protein in myelin. If your T-cells start to react to MBP, it can damage the myelin sheath, cause the myelin to be stripped off, and produce neurological symptoms. This is what happens in animals who get EAE, and the Thai investigators showed that this is also what happens in human patients with SAE. (Figure 5) In this study, the investigators looked at patients who had received the vaccine who did not get any neurological complications in comparison to patients who received the vaccine but did develop neurological complications. They asked the question: “were the responses of the T-cell from these patients different when they put them in a petri dish and cultured them with purified MBP?” The answer was clearly yes. A stimulation index (the details of this index are not important for the purpose of this paper) is used to measure the reactivity of T-cells in response to MBP when you add it to the culture. A stimulation index of 1.0 is normal. So, uncomplicated vaccine recipients did not have T-cells that responded in this type of assay to MBP, but patients that did have neurological complications had active immunological responses to this protein (SI > 2.0). Thus, in some patients, the act of injecting CNS tissue triggered the immune system to respond to MBP. The hypothesis is those myelin specific T-cells then migrated into the nervous system and caused neurological disease. It turns out that not only were T-cells activated against MBP in SAE patients, but also that it caused the production of antibody molecules against this and related proteins. This figure demonstrates that the antibody responses to myelin proteins were higher in patients who developed neurological complications from this vaccine as compared to the patients who did not develop the complications. Those antibodies were present in the blood serum and they were also present in the CSF. Again, the idea is that if you induce these antibodies, that they may enter the nervous system, bind to the myelin that is all over the nerves cells and cause damage that produces neurological symptoms. So, there is something about this vaccine that triggered this abnormal immune response in a subset of patients to cause the disease. In this group of SAE patients, three-quarters of them had antibodies against the MBP molecule. The message is that if your body is triggered to make antibodies to this myelin protein, they have the potential to get inside the nervous system and cause disease. This is, of course, something that we do not want to happen. Understanding these triggering processes is a critical step in being able to intervene early and maybe even prevent these diseases. In conclusion, this vaccine has been shown in a subset of patients to trigger antibody responses and T-cell responses to MBP. We think that is why these patients developed these neurological complications and developed ADEM. Another explanation as to why some patients got SAE and why some patients did not has to do with their genetic background. There are certain types of molecules that are on the surface of all our cells that activate the immune system. These are called HLA molecules and they are very important in turning on T-cells. There are many different types of these molecules, and the type of HLA molecules in my body may be different from the HLA molecules in yours. No one person has all of the types. The hypothesis is that if you have certain types of HLA molecules known as HLA-DR, you may be more or less susceptible to various autoimmune diseases. Again, there are many different types of HLA-DR molecules. These investigators wanted to know, in patients who had received the Semple vaccine, was there a link between certain HLA-DR molecules and the likelihood of getting the disease? It turned out there was such a link. The patients who developed SAE were much more likely to have HLA-DR9 and HLA-DR17 compared to patients who did not get these complications or who did not get the vaccine. The message here is that having these particular HLA-DR molecules may be a disease susceptibility factor. (Figure 7) We are familiar with a similar relationship in MS. If you have certain HLA-DR molecules, you are much more likely to develop MS than if you do not. If we know the subset of people who are more likely to get these diseases, we may be able to identify them and prevent these things from happening. While we are a long way from being able to do this, it is possible that some day we might be able to determine who is more likely to get ADEM following a vaccine, and perhaps not give that type of vaccine to those types of patients. So, understanding these susceptibility factors, and there are many of them in the HLA molecules, is a very important aspect of these studies. We think that if you have these types of molecules, you are more likely to activate the myelin specific T-cells and get the disease. Measles Encephalomyelitis I will turn now to a situation that has more relevance today. Measles is an infectious illness found worldwide. It is a less significant issue in the developed world, largely because of very effective measles vaccines. Still, in patients who contract measles, a small percentage develops ADEM on the heels of the actual infection (Figure 8). This occurs in one out of every thousand cases of acute measles in children younger than two years of age. Furthermore, the ADEM that follows measles infection can be fatal in ten to twenty percent of the patients, and even for those who survive, long-term neurological sequelae are common. In this post-measles ADEM (also commonly called measles encephalomyelitis) there is no evidence that measles virus directly infects the nervous system. In other words, this is not a direct complication of the virus getting into the brain or the spinal cord. When investigators started to study this disease, its pathology looked like an inflammatory demyelinating disease under the microscope. MRI studies also suggested that it had many similarities to CNS inflammatory demyelinating diseases. The hypothesis evolved that for some patients who contracted this virus, the infection triggered an immune response against myelin proteins that produced the neurological disease. As in SAE, those patients who get measles encephalomyelitis also commonly have T-cells that react to MBP (Figure 9). Patients who do not get the disease do not have these cells. Again, the disease somehow triggers these myelin reactive T-cells which, in turn, cause demyelination. We do not yet know how this happens; molecular mimicry is one possible hypothesis. The point is that in a subset of patients, these immune responses are trigger, these activated T-cells go into the nervous system, they damage the myelin, and maybe even the nerves themselves, and they cause ADEM. Conclusions I have discussed similarities between a vaccine-induced encephalomyelitis (SAE), a post-infectious encephalomyelitis (measles encephalomyelitis) and an animal model (EAE). In a subset of patients who are susceptible to these disorders, the immune system is triggered to react to myelin, either by a vaccine or by a virus, and that sets up a cascade of events that causes ADEM. While we no longer use the Semple rabies vaccine in the U.S. and while measles does not often occur in this country, these conditions provide a template to help us study why other infections might trigger an inflammatory demyelinating attack. If we can understand the mechanisms involved, then we may be able to devise more effective treatments that facilitate recovery in patients who develop these conditions or even prevent them from happening in the first place. ADEM is an inflammatory demyelinating disease of the central nervous system. It usually has a monophasic course, and it often occurs on the heels of a vaccine or an infectious illness. We think somehow these disease triggers activate the immune system in an abnormal way to react to myelin, and these anti-myelin immune responses are what drive the disease. So if we can understand the triggering mechanisms and this abnormal inflammatory response, we may be able to block or turn them off to the benefit of our patients. |
{kind=link}
{kind=link}