Volume 8 Issue 1
Fall 2007
Article 2
Demoralization and Depression in Multiple Sclerosis and Transverse Myelitis Johns Hopkins University School of Medicine; Departments of Psychiatry and Neurology; Johns Hopkins TM and MS Centers; The Transverse Myelitis Association Medical Advisory Board Adapted from a presentation at the 2006 Rare Neuroimmunologic Symposium A man walks into a doctor’s office with a duck on his head. The doctor comes out, greets them in the waiting room and asks, “How can I help you?” The duck says, “Can you get this man off my rear end?” This is my daughter’s favorite joke. What often happens for people with depression, as well as cognitive impairment, is that these symptoms can be very subtle. Often, like the doctor in my daughter’s joke, what they believe to be the problem is not what it first appears. Patients often experience a set of symptoms from their condition and my job often involves helping them to see these symptoms in a new light. Sometimes there is an underlying depression involved in the manner these symptoms are experienced. This article will focus on the clinical side of depression. To understand depression, first you have to unlearn some myths, the first being that most people with neurologic illnesses are depressed. “Wouldn’t you be depressed too, if you had MS or TM?” I often hear this from fellow physicians. Not only is this not borne out by clinical and research experience, but this question all too often is used to justify an individual’s suffering and thereby miss an underlying treatable disease. Take the following study as a case and point.
This is an interesting study that came out of San Francisco. In the Mohr study, they made phone calls to people in the community who had multiple sclerosis, and they asked, “How’s it going? What’s going on with your life?” The researchers were able to cluster the responses to these questions into three general areas. One cluster referred to how contracting MS had led to a deterioration in their relationships with their friends and family; that was one in five people. There were 30% of people who responded that they were demoralized in some way. Depression is very common in MS and likely a significant portion of this 30% was people who were depressed. Perhaps most striking, there were 60% of people with MS who said that in some way they had benefited from being afflicted with MS. This meant that somehow the experience of having MS had enriched their lives. There were three times as many people who were enriched by their MS experience as those that complained about troubles with relationships, and twice as many people as those who were demoralized. Is this a surprising result? The following are some of the responses the researchers referred to as benefit-finding (and the percentage of the responses in parentheses). Relationships: My friends and family have become more helpful (77), I am closer to my family (70), I am closer to my significant other (51), I keep in better touch with my family (44). Interpersonal Skills: I have learned to be more compassionate (67), to be more respectful of others (58), express more feelings (55), communicate better (48), be a better friend (48). Perspective: I appreciate the importance of being independent (83), I appreciate life more (74), I am more introspective (72), more conscientious and self-disciplined (60), more motivated to succeed (59), more spiritual (45), more independent in many ways (38), less inhibited (33). I am told all the time by my patients that walking is something wasted on the ambulatory. People do not appreciate the ability to be able to get up and move around. You don’t think about it unless it is something that has been impaired or lost. Most of the studies that have been done are on MS. As you will see from the work we have begun at the Johns Hopkins TM and MS centers, most of the findings reflected in these MS studies also pertain to the whole spectrum of auto-immune conditions, including transverse myelitis, Devic’s and ADEM.
Often when initially confronted with these auto-immune illnesses, the vast majority of people are faced with a tremendous transition in their lives. People who get these disorders often do not know anything about them and they do not know what is going to happen to them. The incomprehensible sense of what the future is going to bring is difficult and makes it a struggle for people to cope. Jerome Frank described and operationalized the concept of demoralization in his work at Johns Hopkins (Frank & Frank, 1993). Demoralization is the state of helplessness, hopelessness, confusion, subjective incompetence, isolation and diminished self-esteem. Demoralization results from a failure to adapt when environmental stress overwhelms an individual’s coping capacity. An individual’s coping capacity is influenced by constitutional variables and resources. The subjective thoughts, feelings, and beliefs of demoralized individuals are that they have failed to meet expectations; their own and/or other’s expectations. They feel overmastered. There is a feeling of being unable to cope with some pressing problem. There are simultaneous feelings of being powerless to change a situation or to extricate themselves from a predicament. There is a sense of isolation; a feeling of being unique and, therefore, not understood. A common subjective experience may be characterized as follows: “I feel awful. No one else understands it. I’m not going to burden anybody else with how I feel. Therefore, I’m the only one who feels like this.” We all have coping strategies that we use to deal with what life throws our way. And, we all have a point beyond which we no longer can cope on our own and become demoralized. We treat demoralization with remoralization. I try to teach this to the residents at Johns Hopkins and to my patients and their family members. A sense of demoralization often results from the accumulation of a number of hurdles that feel insurmountable when taken together. Problem-focused coping skills can instill a sense of mastery. This can be accomplished by breaking down a large problem into smaller and more manageable tasks that can be approached and mastered. When I work with patients with transverse myelitis, I often ask them what kinds of things they are concerned about. I’ve had patients say to me that the worst part of what is going on with them is that they feel as though they’ve lost their independence. For instance, they tell me that they can’t go grocery shopping anymore; that they are just overwhelmed trying to use their walker in the store with all of the people and activity going on around them. I ask them if they can use the cart in the store and if they can go to the store at off hours when it is less busy. If the person can go shopping, this becomes an achievement, which then in turn becomes the start of many future achievements. The journey of a thousand miles begins with a single step. Cumulative small victories can re-instill confidence. Cognitive reframing will help to combat a subjective sense of incompetence and confusion. This involves helping a person think about a problem in a different way: doing a “reality check.” For example, I have had patients come in and say, “I think I’m demented, I can’t remember anything,” by which they mean they used to have all of their friend’s and relative’s phone numbers memorized. I explain to them, “Well, now you will just have to be like the rest of us and will have to write all of these phone numbers down.” The untreatable memory disorder becomes merely an organizational problem. Small achievements will help to combat helplessness, diminished self-esteem and frustrations. Individual and group support and education are also critical components to preventing or overcoming demoralization. Educating yourself is very important as it is often what you do not know that can scare you the most. Once you have information and begin to understand your condition or situation, you can begin to get some control over it. Being a part of a support network helps to combat a sense of hopelessness and isolation. People often need an occasional reminder that it is okay to be merely human. It is important for a person to have a chance to express their feelings in a nonjudgmental setting.
Cody has overcome some tremendous hurdles; she has made peace with her illness. Cody’s quote reflects the end result of someone who has found their way through and out of demoralization. Cody embodies the spirit of what it can be like to truly overcome the obstacles of demoralization and disability and emerge invigorated. The issue of the caregiver’s wellbeing in chronic illnesses is poorly studied in the medical literature, it is not sufficiently focused on and it is critically important. It is difficult to have one of the neuroimmunologic disorders; it is much harder than difficult to have one of these disorders without a healthy caregiver. When I first see a patient with transverse myelitis, I spend at least a third of the time talking to their caregiver. I talk to them separately to touch base with them to see how they are doing. This generally doesn’t get done in the medical setting despite its importance. I have found that the health of my patients is critically dependent on the wellbeing of their caregivers. In a number of studies, caregivers report that there are both positive and negative aspects to being a caregiver. Patients generally underestimate the level of distress that their caregivers are having. In other words, and for obvious reasons, the patients tend to focus on their disease, as the doctors do, and not focus on the caregivers. The wellness of the caregiver is often neglected. Caregivers report an increased frequency of loss, loneliness and isolation. Caregivers often offer me a justification for not attending to their personal wellbeing with explanations such as this: “Of course I don’t have friends any longer and I don’t go out anymore, because I am so busy taking care of my loved one.” While a person has the disease in their body, transverse myelitis and related neuroinflammatory disorders affect the whole family. The family and the patient are all in this together. If the person who has the disorder is going to do well, the caregiver and the rest of the family also have to do well. Caregiver and care recipient coping strategies should be complementary; there is more than one way to adapt together to life under altered circumstances. It helps to have problem-focused coping skills. Both the caregiver and the care recipient have to come to terms with and accept what things they cannot change, to have the courage to change the things they can, and the wisdom to know the difference. If the care recipient or the caregiver becomes increasingly distressed, then something new has to be tried. It is important to know when and where to intervene and not to get stuck in a failed strategy. I had a patient with transverse myelitis who was a doctor and his wife a nurse. Doctors are, in general, the worst patients in the world. He told me that he felt like he was burdening his wife. She wanted to help; he didn’t want to let her help. That was a failed strategy. She felt really hurt. He needed to let her help so that they could be working on the problems together. As soon as he let her do this, they became one another’s ally. It is important not to get stuck in failed strategies. It is critically important that the caregiver realize that they have to take care of themselves in order to be available to take care of their loved ones. Studies indicate that caregivers’ health often suffers, because they don’t go to their own doctors regularly and don’t take as good care of themselves. Taking care of the caregiver’s needs does not conflict with the care recipient’s needs. It is not taking time away from their loved ones and it is absolutely essential that they take care of themselves. When you get on an airplane, the flight attendant explains that should the cabin lose pressure and the oxygen masks drop down, parents traveling with small children should put their own mask on first and then take care of their child. I know a caregiver is in trouble when I ask them who they would put the mask on first; themselves or their child and they tell me, of course, their child. I explain to them that when the oxygen gets sucked out of an airplane, you have about 20 seconds before everybody loses consciousness. If you are there fighting to get the mask on the child and you don’t succeed in 20 seconds, the kid is not going to make it because you are not going to make it. If you put it on yourself first, you have the opportunity to eventually put it on the child. After explaining this to the loved ones of my patients, I ask them when they come back for appointments, “Are you getting enough oxygen?” Are they making the time and the effort to take care of themselves? They need to ensure that they have a chance to recharge their energy and do not become burned out. Major depressive disorder is different from demoralization. I was listening to sessions at the 2004 Neuroimmunologic Symposium and someone called me over to ask me a question. She did not know that I was the neuro-psychiatrist at the conference. She had been listening to a day of lectures and she asked me, “When is someone going to get up and explain and talk about how having transverse myelitis is like being dead while you are alive? When are we going to get to that?” I said, “I’ll get to that, just hang on.” We have known about depression since Hypocrites. Hypocrites called it melancholia, which literally translated means black bile. As far back as the ancient Greeks, it was considered one of a number of medical conditions. They did not differentiate between melancholia and any of the other possible ailments. It was a medical illness that needed to be diagnosed and treated. There was little stigma associated with it at this time; nothing like what has arisen today. There are so many myths and misunderstandings about depression. Much of what people think they understand about depression is not correct. People who have had depression and had it treated do understand it. One of my patients told me, “Dr. Kaplin, I’m starting to get depressed again. I’ve had open heart surgery and I’ve been depressed and I’d rather have another open heart surgery than go through depression again.” If that does not register with you than you probably have not had depression and not had it treated successfully.
The brain has numerous functions. It is not hard for people to understand that the brain controls nerves that wire our muscles and that when people have MS or TM, the muscles may not work as they should. It is not hard for people to understand that you could have troubles with these illnesses that could affect your brain and lead to trouble with memory and concentration. People do have a difficult time understanding that there is a part of the brain that regulates our moods. There is a mood thermostat in the brain and when it gets stuck, people get depressed. If the thermostat in a room got stuck on low, it would get colder, and colder, and colder and nothing would raise the temperature and make it hotter. It is that unresponsiveness that is one of the hallmarks of depression: a fixed, unresponsive low mood. We know that there is a biology to depression. We can actually measure changes in the brain. There are certain regions in the brain of untreated people who are depressed that shrink approximately 20% in size. It turns out that depression is toxic to your brain. The measure of changes in people’s rapid eye movement during sleep and the cortisol suppression test demonstrate that there is a real biology involved in depression. One of the best examples of the existence of this mood thermostat was discovered in doing deep brain stimulation to treat patients with Parkinson’s disease. There is a very interesting case where they accidentally place the probe in a region that turned out to be wired to this mood thermostat. Every time they turned on the stimulus, this woman would start crying and have this sense of overwhelming doom that would possess her. She would ask them to turn off the electrical stimulation. When they would turn it off, she would suddenly feel fine again. They had placed the electrode right into the central pathway of a mood thermostat, turned it on and she got all of the symptoms of depression.
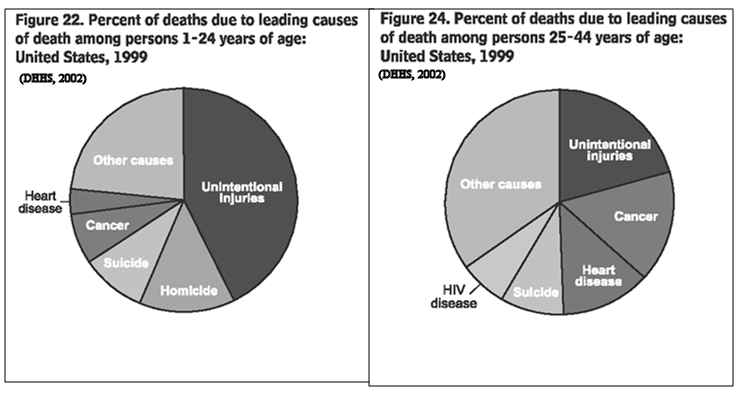
Lou Gehrig’s disease or ALS is arguably one of the worst diseases. In most cases, death occurs from about six months to a year of diagnosis. Death often results from becoming completely paralyzed and on a ventilator and very susceptible to pneumonia. It is a terrible disease. ALS affects the nerves that wire the muscles; they stop working and muscles cannot be controlled. ALS does not directly affect the brain. It is a motor neuron disease. The rate of clinical depression in ALS patients is rare. They do not have depression at any greater rate than anybody else in the medical setting, such as people with colds or the flu. They can become demoralized and have a difficult time with the disease, but they do not get the constellation of symptoms that we call clinical depression. They may feel that, “this is a terrible situation I am in, this is awful,” but they do not tend to get the kind of situation where they say, “I am awful, I deserve this and I don’t even want to hang in there for six more months.” One of the things that is always interesting and ironic to me is that sometimes people with MS and TM tell us that it took them a long time to convince their doctor that there was really something wrong with them; that the symptoms of weakness, numbness, dizziness are real and should not be dismissed as just something “in your mind.” Then I have to convince people who have symptoms of clinical depression after they get MS or TM that these are not just all in your mind, they are in your body, they are in your brain. Depression is not a “state of mind” or a weakness or a character flaw. Depression is part of the disease, part of your multiple sclerosis, part of your TM. You can get spasticity, you can get urinary problems, you can get depression. There are many conditions that will cause depression, but transverse myelitis and multiple sclerosis are the record holders. There are higher rates of clinical depression in TM and MS than in any other conditions. MS has the highest rates of depression ever described, and that is because this condition attacks the brain in a specific way, and that attack leads to depression. According to former Surgeon General Satcher (1999), “Far more Americans die from suicide than from homicide.” Suicide is the 3rd leading cause of death in the general population for ages 1-24. It is the 4th leading cause of death in the general population for ages 25-44. And suicide is the 1st leading cause of death in physicians ages 25-44. Suicide is a major public health issue. Depression is the single best predictor of cardiac mortality within 12 months following a heart attack. Depression is probably bad for the heart, because it is bad for the neurons that control the autonomic nervous system that controls the heart. Depression is also the second leading cause of chronic disability.
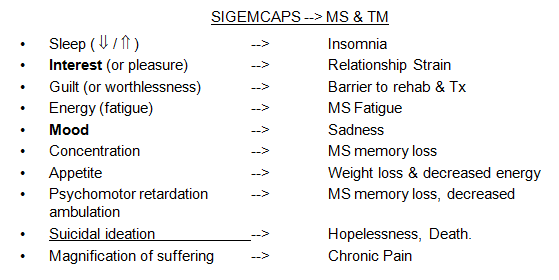
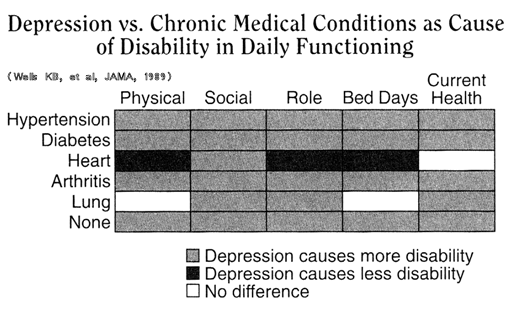
This chart compares hypertension, diabetes, heart disease, arthritis, and lung disease to depression. The black cells mean that the medical disease caused less disability when measured in these five different ways, gray means the depression caused more disability and white means that they broke even. Heart disease is the leading cause of chronic disability and depression comes in second. If depression does not kill you, and hopefully it won’t, it certainly is the cause of major disability. There are two simple myths that are used inappropriately to dismiss the diagnosis of depression. What often happens is that a physician will think that a patient is not depressed; they are stressed. They tell me, “You would be stressed, too, if you had their condition. You do not know when the next attack is going to come. You do not know if you are going to get better from the symptoms.” When I persuade the physician that the patient is depressed they say, “Okay, sure they are depressed. They will get over it.” The problem is that stress does not prevent you from getting depressed. In fact, stress is a risk factor to getting depressed. Stress does not mean you will not get depressed; it means that you are more likely to get depressed. In TM and MS there is no correlation between clinical depression and disability. People with more severe physical functional deficits are not more likely to be depressed than people with less severe deficits. Depression correlates, rather, with number of attacks or the severity of the attacks on the nervous system of the immune system. Depression is not normal sadness. If you are not sad at some point during the course of your life, you are not paying attention to what is going on around you. Sadness is an intermittent and universal experience. That is depression with a small “d”; it is normally responsive to the environment. The degree and duration of the sadness is appropriate to the stressor and it doesn’t unduly disrupt work or social function. It is the lack of responsiveness that is critical. Major depression is a syndrome; it is not just severe sadness. Sadness is to major depression what cough is to pneumonia. By way of analogy, I tell my clinical colleagues that a cough can be an indicator of pneumonia and sadness can be an indicator of depression; it is just one symptom. Not every cough is the result of pneumonia. Sometimes pneumonia presents without a cough. You could get depression without sadness, particularly in kids. Instead of sadness, you might see irritability. You have to consider the company the cough keeps. If it is a cough with a set of symptoms (productive sputum, tachypnea, fever, consolidation), then we call it pneumonia. There is a set of symptoms that we call depression. The acronym SIGEMCAPS is used in medicine to remember them. For a diagnosis of depression, you need to have at least decreased interest (or pleasure) or decreased mood and then a total of five of these nine symptoms (for more than two weeks): trouble with sleep (either increased or decreased), loss of pleasure (your get-up and go has gotten up and gone), feelings of guilt or worthlessness, low energy or fatigue, low mood, decreased concentration, increased weight (chocolate for women is what they tend to tell me does it when they are depressed), or loss of weight, psychomotor retardation (or agitation) and then suicidal ideation or thoughts of death. The more symptoms you have, the more likely you are to respond to treatment. If you are not sure whether you are depressed, you can ask your spouse; they will tell you. More often than not, it is the spouse that sends people in to see me. When a person is depressed, they don’t want to burden anyone or want other people to know. When they are out in public, they put on their best face and try to mobilize what resources they have. That takes a tremendous amount of energy to do while depressed. To make yourself look happy when you are really depressed takes an immense amount of concentration and effort. Then when they go home, they have to stop trying. It is like having run four-minute miles all day long. They get home and have to just relax. They let their guard down and the family sees what they are, which is depressed. So the family often takes the brunt of it. Jean-Martin Charcot (1825-1893) is the first person to describe multiple sclerosis. The very first patient that he ever described in lectures that he gave to medical students on the diseases of the nervous system in 1868 was a 31 year old woman. Mademoiselle V. experienced periods of serious depression accompanied by paranoia that made her think that Charcot was trying to poison her. In fact, her depression was so severe that she stopped eating and had to be fed by a stomach pump to keep her alive. That is the very first patient who was ever clinically described to have multiple sclerosis. We have known about depression associated with these conditions back to the very first patient described, but ironically, it was not until the last 10 or 15 years that depression has been studied in MS. Burden of Depression in MS Patients (Patten & Metz, Psychother Psychosom, 1997, 66:268-92) Lifetime Prevalence: Current Prevalence: The available evidence suggests that depression in MS is caused by the effects of inflammatory insults to the brain. It is just like the other symptoms that you get with MS, like the tingling when you put your chin on your chest, for those people who get L’Hermitte’s sign. It is one of the set of symptoms that happens when your brain is under attack. Depression does not correlate with physical disability. It tends to occur during periods of time of inflammation. Periods of immune activation correlate with increased rates of depression and suicide. Multiple studies have shown that depression is the primary determining factor in patient’s self reported quality of life, with greater impact than other variables investigated, including physical disability, fatigue, and cognitive impairment. Depression also has a significant affect on function. Depression is the primary determining factor in the quality of relationship when rated both by patients and their significant others. Depression is associated with disruption of social support, increased time lost from work, and decreased adherence to neuromedical treatment regimens for MS.
Depression also worsens cognition. Some degree of cognitive impairment occurs in 50% of MS patients. We also find high rates of cognitive impairment in transverse myelitis. This impairment includes memory recall, information processing speed, executive function and working memory. Cognitive deficits are found in moderate to severe depression. Performance in depressed MS patients may be normal for routine tasks but impaired on tasks involving effortful attention. Depression in MS is associated with impairment of complex speeded attention, planning and working memory. Impairment can wax and wane with the type of task and mood. Both MS and depression have overlapping cognitive deficits. The combination of the two is additive in resulting impairment. The important thing to know is that if you have one cause, it does not help to also have another cause. Often patients come in and I tell them, “I understand you’re having trouble with your concentration. I don’t know if it’s the depression or the MS.” You don’t know unless you get the depression out of the way by treating it. Depression is strongly associated with the impact of fatigue on the lives of MS patients. Disabling fatigue almost always interferes with activities (Chwastiak, et al, 2005 JPR). Auto-immune fatigue tends to hit at about 2:00 or 3:00 in the afternoon. In the morning, you wake up feeling better, and as the day goes on, you get more and more fatigued. Then by 2:00 or 3:00 you hit the wall and you feel you cannot take another step. That is classic MS fatigue. Not everyone has classic auto-immune fatigue. MS patients with depression are six times more likely to report disabling fatigue. Fatigue with depression is the reverse of MS fatigue. The fatigue is often worse in the morning and better at night.
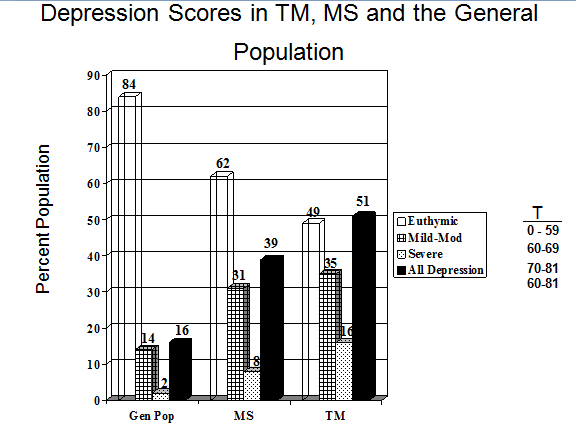
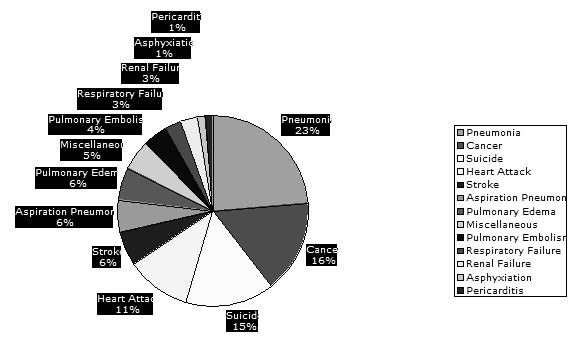
There is a 30% lifetime incidence of suicidal intent (thoughts of wanting to kill oneself) in MS. 6% to 12% of patients with MS attempt suicide. Suicide was the 3rd leading cause (15%) of death in 3000 outpatients in Canadian MS clinics from 1972-1988. MS patients dying from suicide were younger and less disabled than patients dying from pneumonia (23%) and cancer (16%). (Sadovnick, et al, 1991, Neurology). Of 750 transverse myelitis patients at the Johns Hopkins TM Center, 60% of the deaths have been from suicide. It is the number one cause of death in TM. It is like smoking; depression is the most preventable cause of death in transverse myelitis. It is severe. Suicide is the third leading cause of death; pneumonia and cancer are numbers one and two. Pneumonia and cancer tend to occur in the elderly. If someone is going to die relatively young, it is more likely going to be from suicide. These are results from the TM Center at Johns Hopkins. The bars with dots are severe depression and the bars with cross hatch are mild depression. Depression in MS is higher as compared to the general population and transverse myelitis had at least equal if not greater rates of depression than MS. We began to suspect that there might be brain involvement in transverse myelitis.
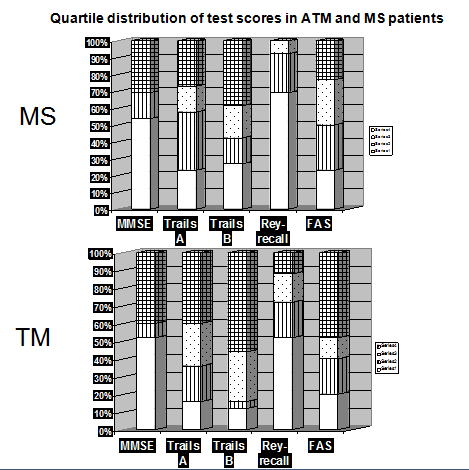
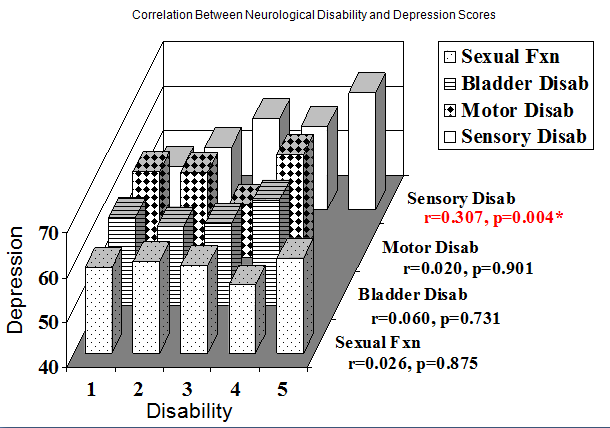
Quartile distribution of test scores in ATM and MS patients The white portion of the bar (bottom) signifies a problem; the higher the white portion, the worse the patients scored on these tests of memory and concentration. We saw the exact same pattern in patients with transverse myelitis. They had the same memory problems that you see in MS. We now understand that the immune system is attacking the brain in transverse myelitis even though we don’t see the lesions on the MRI. Evidence suggests that the activated immune system that has gotten into the brain and spinal cord is pumping out all of these chemical messengers, and those chemical messengers cause the depression. We found that depression does not correlate with motor disability, bladder disability or sexual function in patients with TM. There was a mild correlation that accounted for 10% of the variability in pain; the worse your pain, the worse your depression scores. That may be because people who are depressed have worse pain or maybe the people who have worse pain, have worse depression. The two go hand-in-hand.
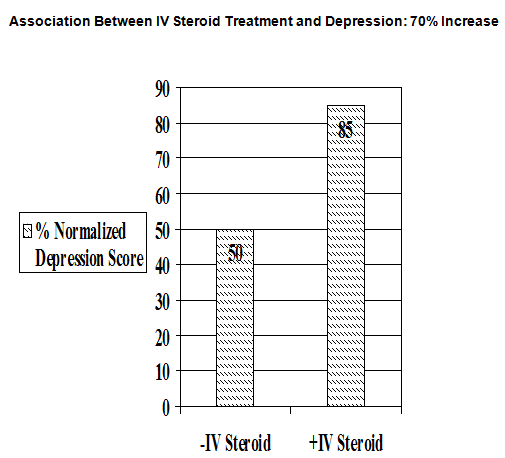
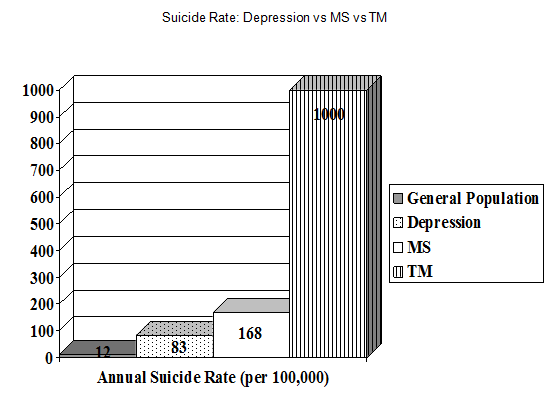
Giving steroids during an acute attack of TM involves a risk benefit analysis. The benefit of giving the steroids is that they may arrest the inflammatory attack and spare the nervous system damage. There could also be side effects from taking the steroids. In patients with transverse myelitis, those people who had received IV steroids at the time of their initial presentation were 70% more likely to have depression at some point in the future. It may be that those were the people who were depressed when they came in to their doctors and they looked really bad so they got steroids. We cannot prove this; it wasn’t a prospective trial, but it is just worth mentioning that we know from other studies that steroids can increase your chances of getting depressed. If you already know steroids make you depressed, then tell your doctor. They may have great benefits and you should do it, but it may have risks. This graphic shows the rate of suicide in depression, the rate of suicide in MS and the rate of suicide in transverse myelitis
Chronic stress has been linked to increased risk for MS exacerbations, as well as accrual of disability (Mohr, et al). A prospective, longitudinal investigation involving serial imaging using MRI with gadolinium enhancement demonstrated that stressful life events (especially family conflict and work-related stress) predicted the development of new and active brain lesions. A meta-analysis of studies examining the effects of stress on MS exacerbations found a significantly elevated risk of exacerbation associated with stressful life events in 13 of the 14 investigations. The degree that stress increased the risk of MS exacerbations in this meta-analysis was on average 60% greater than the degree that IFN-beta treatment has been shown to decrease the risk of MS exacerbations. Chronic stress, such as that caused by depression, tends to increase your chances of having worsening of your MS or transverse myelitis. Often when a patient is sent to me, they have been through the process of trying to find a doctor who can figure out a diagnosis of MS and TM. Because they were not sleeping, they were given benzodiazepines, such as valium, to help with the sleep. But because they were also fatigued, they were given Provigil and the Provigil worsens their sleep. So they have to get a higher dose of benzodiazepines. They had concentration problems in part from the MS, and perhaps in part from the depression, and now the benzodiazepines make them feel drunk. If you take enough valium, you will have trouble with your concentration, as well. One of the things I often do is try to detoxify people from what their doctors have placed them on through the process of treating individual symptoms and missing the diagnosis of the underlying depression. If you try to treat depression symptomatically, you will make people worse. On the other hand, if you treat the depression, you may actually make the MS better. This was demonstrated in the Mohr study (Mohr et al, 2001, Arch Neurol, UCSF). Patients with depression had biological evidence of worse MS disease severity. In patients who had depression, their immune system, as measured in the laboratory, was twice as active and aggravated as the patients who were not depressed. Treatment of depression in MS patients (with either medication or psychotherapy) correlated with improvement in their autoimmune disease status. This suggests that the treatment of depression may be an important component in the management of MS. As the authors state, “Treatment of depression may provide a novel disease-modifying therapeutic strategy as well as a symptomatic treatment for patients with MS.” Stress has been linked to increased risk for MS exacerbations, as well as accrual of disability. You should get treated not just for yourself, not just because your family deserves you to get treated if you are depressed, but you should get treated, because it may very well impact significantly on the course of your disease.
The good news is that depression is the most treatable syndrome associated with MS. My neurology colleagues sometimes tell me how jealous they are when a patient comes to me who is not working, been in bed for a month, having a horrible time of it, family does not know where they went, this is not the person I married, this is not the mom and dad I remember, they have changed dramatically. I treat the depression and in a month they are back at work, they are doing great. The neurologists are ordinarily not able to be as effective in treating the other symptoms that come with MS and TM, such as fatigue, nerve pain and spasticity. Depression is by contrast very responsive to treatment. No pill can help me deal with the problem of not wanting to take pills; likewise, no amount of psychotherapy alone can prevent my manias and depression. I need both. It is an odd thing, owing life to pills, one’s own quirks and tenacities, and this unique, strange, and ultimately profound relationship called psychotherapy. This is a quote from one of my mentors, Dr. Kay Redfield Jamison. She dealt with having a terrible illness. She went to her chairman and said, “I know you are going to fire me. I have bipolar disorder. I have a crazy psychotic mania.” He told her that he wasn’t going to fire her. His advice to her was, “learn from it, write from it, teach from it.” She is a better clinician and researcher today, because she has bipolar disorder. Again, you can utilize these things and often turn them into benefits. Depression and MS is a two-way street. MS causes depression, depression and stress worsens MS. Treating the depression improves the MS. We looked at the data to demonstrate that improvement. Treating the MS improves depression. We do not yet have the studies showing that improvement. I would like to pursue those studies. Depression is a lethal consequence of MS if untreated. Depression is common in these autoimmune diseases, it is caused by the immune system and it is treatable. Paula Lazzeri is also one of my mentors. Paula got TM as a child and was paralyzed from the chest down. Paula graduated from college with a degree in accounting and works full time. She married a wonderful man who became a physical therapist as a result of being so inspired by his wife. Paula and Myk have a beautiful son. Paula carried and delivered this child with her paralysis. Paula is also an officer in The Transverse Myelitis Association and devotes a significant part of her life helping others. Paula made the following statements in a speech she gave at the 2004 symposium.
Paula is the best example of how you can overcome the demoralizing effects of these illnesses. However, if you are depressed, you cannot follow Paula’s example. Hearing about Paula for people who are depressed only makes them feel worse. They think, “I’m a wretch and how did she do all of that? And I can’t do that?” The problem is Paula is fabulous and for those of you who are demoralized, talk to Paula. Those of you who are depressed, talk to me, because poor Paula cannot help you. I will tell you that you can become Paula, if you get the depression out of the way.
Depression is treatable. Your life could be so much better if you get your depression out of the way. Do not settle for this is the best my life could be unless you have really excluded all of the possibilities. |
 .
.